This is a website for healthcare professionals.

AVISE HCQ
A whole blood test to measure hydroxychloroquine (HCQ) levels
AVISE HCQ provides accurate measurement of drug levels to help inform personalized therapeutic decisions.
ADVANCE YOUR INSIGHT WITH AVISE THERAPEUTIC DRUG MONITORING
AVISE HCQ is an advanced drug monitoring test that provides an accurate measurement of HCQ levels in whole blood to help physicians assess their patients' exposure to HCQ therapy (PLAQUENIL). Continued monitoring, allows for precise dosing to make sure a patient’s symptoms are being managed without putting them at risk for complications that are caused by too little or too much HCQ.

Respond to your patients with greater insight
AVISE HCQ is intended for use in patients on PLAQUENIL therapy, after steady state (approx. 90-120 days), to help assess the following:
- Patient compliance
- Patient risk for disease flares
- Therapeutic decision making
- Individual metabolism
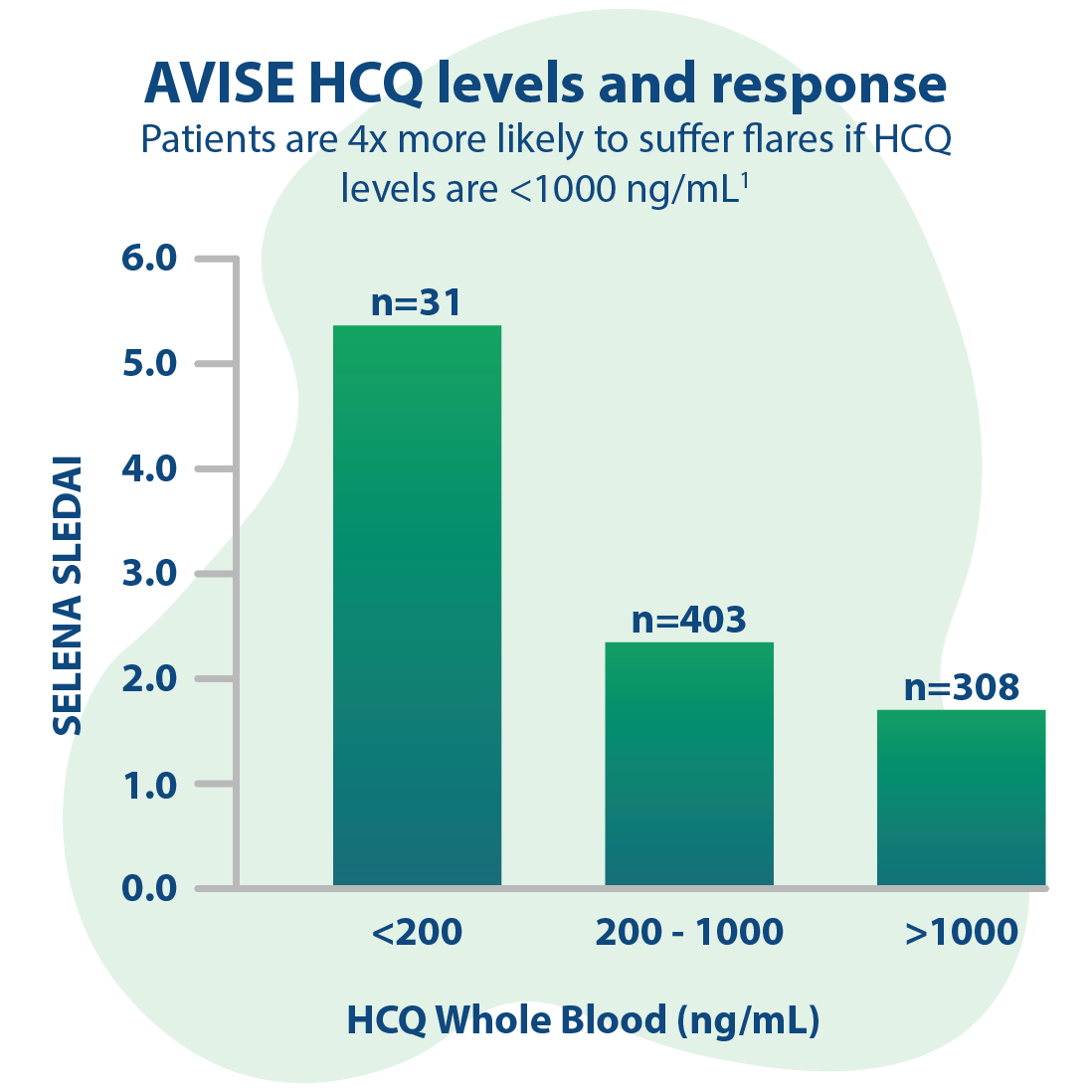
Evaluate a patient’s risk for disease flares
HCQ can calm an overactive immune system. It is thought to work by interrupting some of the signals that activate the immune system and reducing the amount of pro-inflammatory chemicals that are released by immune cells.1 For people with autoimmune disorders, HCQ can be an effective way to manage their symptoms.

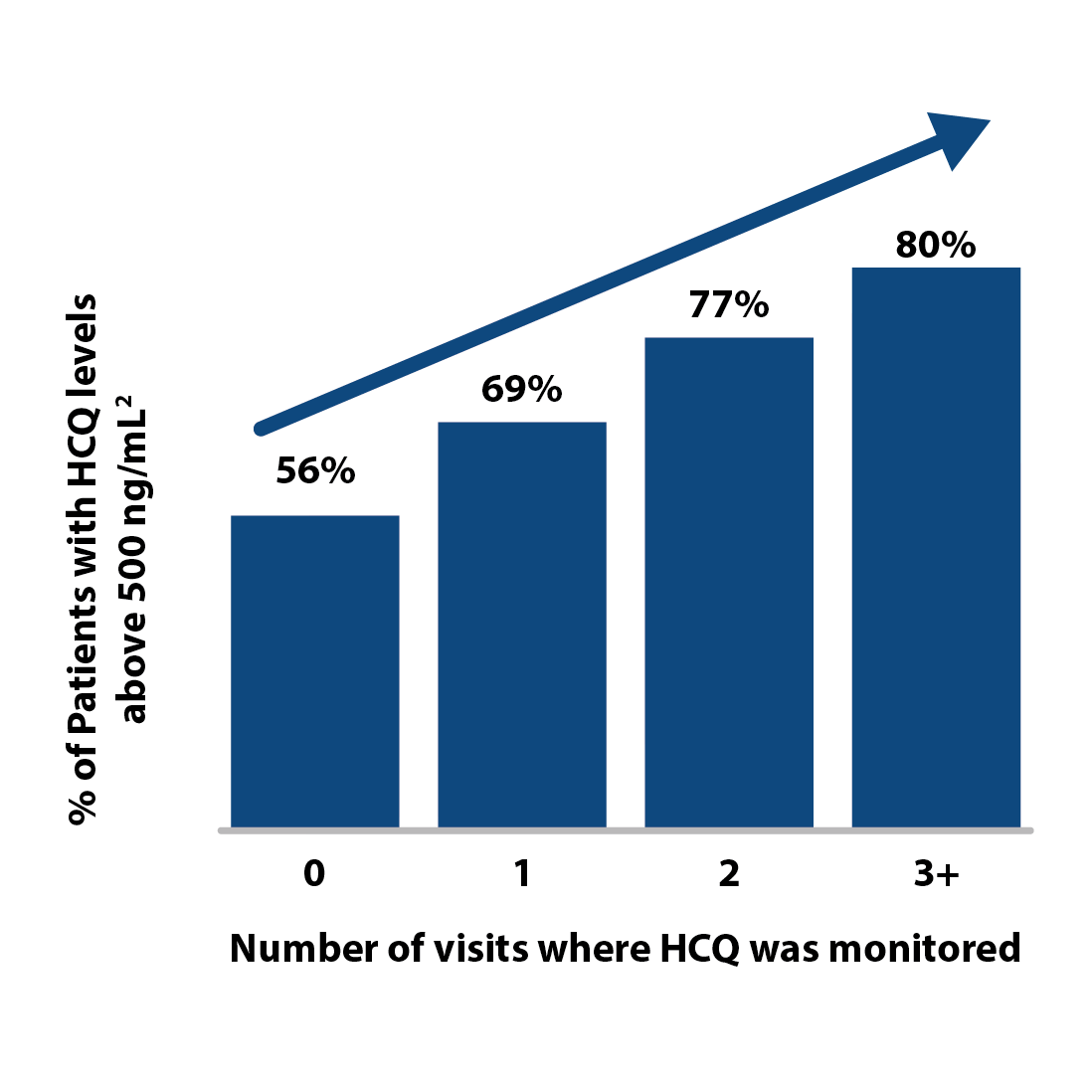
Address patient compliance and response
HCQ is generally safe when used as directed, but it’s important for individuals taking this drug to be aware of the signs of toxicity and the dangers of overdose. People who take large doses or who use HCQ for a long time are at particular risk for toxicity, since this drug accumulates in several organs, including the eye, the skin, and the liver. Regular blood testing gives doctors a way to identify the lowest effective dose and tailor it as needed to ensure that patients get the best outcomes with the lowest risks.

References:
-
Costedoat-Chalumeau N, et al. (2013a) Hydroxychloroquine in Systemic Lupus Erythematosus: Results of a French Multicentre Controlled Trial (PLUS Study). Ann Rheum Dis 72:1786-1792.
- Durcan L, et al. Hydroxychloroquine Blood Levels in Systemic Lupus Erythematosus: Clarifying Dosing Controversies and Improving Adherence. The Journal of Rheumatology. 2015.